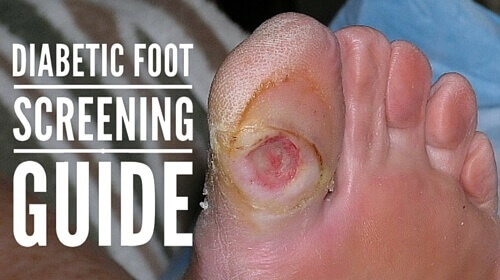
Five clinical tests for diagnosing loss of protective sensation in the diabetic foot, plus tips on inflammation assessment.
How serious are diabetic foot ulcers? The statistics are sobering:
- It is estimated that between 10 and 25% of patients with diabetes will develop a foot ulcer in their lifetime.
- Diabetic foot ulcers precede 84% of all lower leg amputations.
- The five-year mortality of patients with newly diagnosed diabetic foot ulcers (DFUs) is nearly 50%, and carries a worse prognosis than breast cancer, prostate cancer, or Hodgkin’s lymphoma.
In addition, DFUs are at increased risk for infections and other complications, and continue to be a major cause of hospitalizations and additional healthcare expenditures. So while patients suffer greatly from DFUs, these chronic wounds are also a huge financial burden on healthcare systems. This is because these same patients spend more days in the hospital, and experience more visits to the emergency room and outpatient physician offices than other patients with diabetes.
The importance of diabetic foot screening and assessments
As a healthcare clinician, it is very important to complete a comprehensive assessment and diabetic foot screening with all diabetic patients. This assessment, as recommended by international and national diabetes clinical practice guidelines (CPGs), is critical to the prevention of foot complications people with diabetes.
The American Diabetes Association recommends that all individuals with diabetes should receive an annual foot examination to identify high-risk foot conditions.This examination should include assessment of protective sensation, foot structure and biomechanics, vascular status, and skin integrity.
Five clinical tests for diagnosis
The task force of the Foot Care Interest Group of the American Diabetes Association recommends the use of five simple clinical tests for diagnosis of loss of protective sensation (LOPS) in the diabetic foot:
1. 10-gm monofilament
The filament is applied perpendicular to the skin with a slight pressure until there is an obvious bend of the fiber. The patient then provides verbal feedback when the sensation is perceived.
2. Vibration using 128-Hz tuning fork
Strike the tuning fork against the palm of your hand and then apply the base of the tuning fork to the patient’s forehead or sternum. Ensure that the vibration sensation (not just the touch sensation) is understood. Apply the tuning fork to the dorsum of the first toe just proximal to the nail bed. Ask if the vibration sensation is perceived.
3. Pinprick sensation
A disposable pin is applied just proximal to the toenail on the dorsal surface of the hallux, with just enough pressure to deform the skin. Inability to perceive pinprick over either hallux would be regarded as an abnormal test result.
4. Ankle reflexes
Using a tendon hammer, perform the ankle reflexes test with the patient either kneeling or resting on a couch/table. The Achilles tendon should be stretched until the ankle is in a neutral position before striking it with the tendon hammer. If a response is initially absent, the patient can be asked to hook fingers together and pull, with the ankle reflexes then retested with reinforcement. Total absence of ankle reflex either at rest or upon reinforcement is regarded as an abnormal result.
5. Vibration perception threshold testing.
The hand held biothesiometer device gives a semi-quantitative assessment of vibration perception threshold (VPT). With the patient lying supine, the stylus of the instrument is placed over the dorsal hallux and the amplitude is increased until the patient can detect the vibration; the resulting number is known as the VPT. This process should initially be demonstrated on a proximal site, and then the mean of three readings is taken over each hallux. A VPT >25 V is regarded as abnormal.
Inflammation assessment
During a diabetic foot screening, clinicians should assess for inflammation using an infrared dermal thermometer. A >2-3°F increase of an affected site as compared with an unaffected site is considered significant for inflammation. In addition:
- Warm areas or hot spots outside this range indicate inflammation, which may be due to infection, fracture, Charcot’s osteoarthropathy, or soft tissue trauma.
- An area of increased localized skin surface temperature (2-3˚F) around a wound compared with a mirror-image temperature can indicate deep and surrounding infection.
- Limb ischemia results in lower regional, local, and side-to-side variability in temperatures. Using the handheld thermometer, the operator is able to essentially map out an unequal vascular supply by measuring the temperatures proximal and distal to the wound.
- Noncontact infrared thermometers can detect localized increases in skin surface temperature comparable to scientific grade instruments.
- People with one or more high-risk foot conditions should be evaluated more frequently for the development of additional risk factors.People with neuropathy should have a visual inspection of their feet at every visit with a health care professional.
Are you ready to assess?
Complications of the diabetic foot are common, complex and costly. This is why healthcare clinicians must administer aggressive and proactive preventative assessments. It’s also why advanced training, such as the WCEI’s Diabetic Wound Management certification course, can make a big difference.
In the meantime, we’d love to hear from you: what are your thoughts about the diabetic foot ulcer assessment and screening processes outlined here? What challenges do you face when assessing, and what have you experienced with your patients as a result of your screening process? We are interested to read your stories – please leave your comments below.
Wound Care Education Institute® provides online and onsite courses in the fields of Skin, Wound, Diabetic and Ostomy Management. Health care professionals who meet the eligibility requirements may sit for the prestigious WCC®, DWC® and OMS national board certification examinations through the National Alliance of Wound Care and Ostomy® (NAWCO®). For more information see wcei.net.
What do you think?