
Diabetes doesn’t just affect blood sugar — it can silently reshape the feet, leading to chronic wounds that resist healing. In this quarter’s WCEI Buzz Report, we explore how minimally invasive surgery (MIS) is becoming a game-changing solution in diabetic foot deformities, helping to prevent amputations and restore mobility.
According to the American Diabetes Association (ADA), approximately 11.6% of Americans live with diabetes. Roughly one in four people with diabetes will develop a foot wound in their lifetime, and someone in the world loses a lower limb due to diabetes-related complications every 20 seconds.
Understanding the root cause of foot deformities
Diabetic foot ulcers (DFUs) often develop due to a combination of neuropathy, reduced blood flow, trauma, and foot deformities. Motor neuropathy plays a significant role by weakening muscles and altering joint stability, which shifts pressure points within the foot. This makes it difficult for diabetic patients to wear properly fitting shoes, contributing to callus formation and ulcer development.
Although conservative approaches like diabetic shoes, inserts, and routine podiatric care can help, they’re not always enough. When deformities persist, surgical correction may be necessary.
Small incision, big impact
MIS limits the size of incisions to five millimeters or less, guided by imaging and specialized instruments, to correct structural foot deformities with minimal disruption to soft tissue. The result: lower inflammation, fewer infections, and faster recovery. By relieving pressure caused by deformities at ulcer sites, MIS improves healing and reduces recurrence.
Toe deformities and the link to ulcers
Toe deformities are common in diabetic patients and significantly raise the risk of pressure wounds. Fortunately, MIS can safely correct these issues while promoting faster healing. Here are three of the most common:
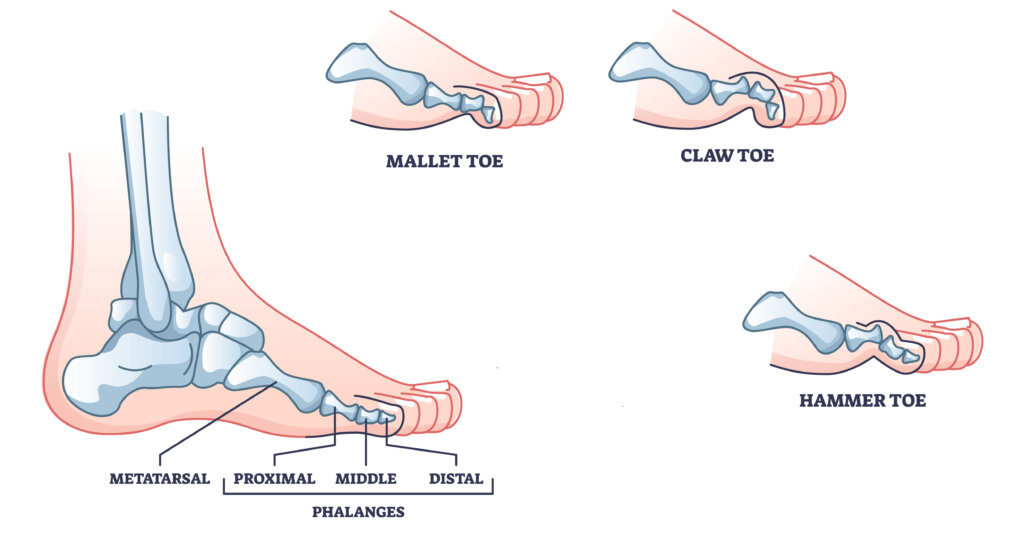
- Hammertoe: The second, third, or fourth toe bends abnormally at the middle joint, forming a hammer-like shape. Pressure builds at the tip and top of the bent joint, leading to calluses and wounds.
- Claw toe: This deformity features an upward bend at the base of the toe (MTP joint) and downward bends at the middle and tip joints. These pressure points can lead to ulcers and put patients at greater risk of infection and even amputation.
- Mallet toe: This affects the joint closest to the toenail, causing the tip of the toe to point downward. This often results in callus formation and pressure wounds.
Toe deformities can be classified as flexible or rigid. Flexible foot deformities can sometimes be corrected with soft tissue procedures like flexor tenotomy (tendon release), which releases tension and offloads pressure. Rigid deformities typically require bone realignment through a procedure called minimally invasive percutaneous surgery (MIPS).
MIS techniques such as percutaneous tenotomy, phalangeal osteotomy, and capsulotomy are performed through small incisions (one to two millimeters). These procedures reduce trauma to surrounding tissue and can be performed under local anesthesia, making them ideal for high-risk diabetic patients.
A study in Foot & Ankle International reported high healing rates with percutaneous tenotomy for diabetic toe ulcers, supporting the safety and effectiveness of MIS.
Healing bunions to heal the wound
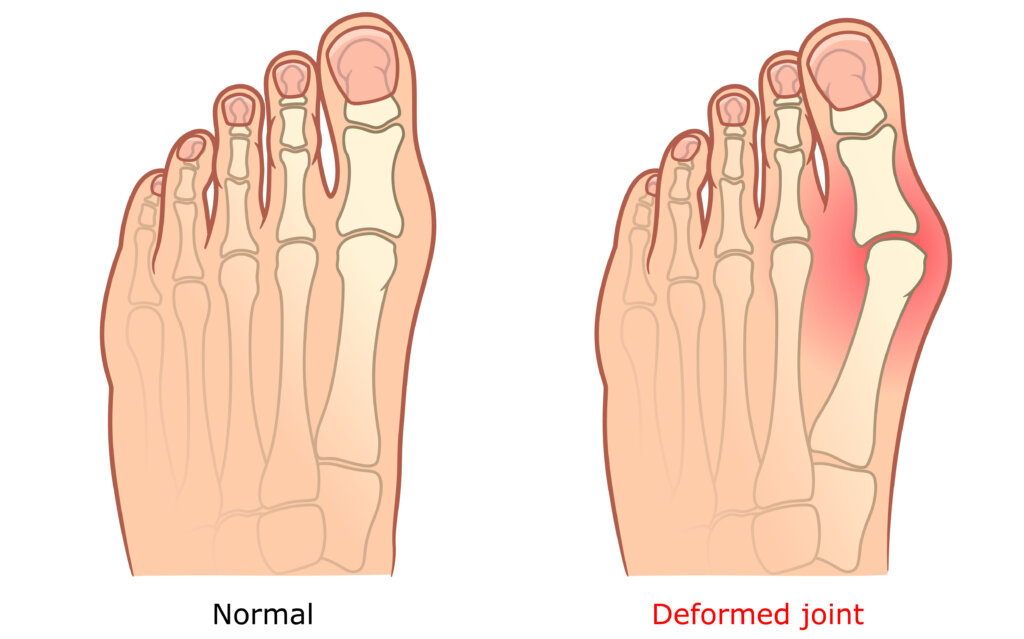
Bunions (hallux valgus) in diabetic patients can create abnormal pressure over the big toe joint, especially when combined with neuropathy and poor healing. This often leads to ulceration over the bunion area.
A percutaneous bunionectomy, a minimally invasive technique to realign the first metatarsal, can relieve this pressure and promote healing. Often performed under local anesthesia, this procedure is safer for patients with additional health risks.
Benefits of MIS for bunions include:
- Corrects or reduces foot deformities
- Promotes faster healing
- Reduces infection and amputation risk
Research published in Foot & Ankle Orthopaedics confirms that diabetic patients undergoing this procedure show improved foot function and ulcer healing, with complication rates similar to non-diabetic patients.

MIS for plantar metatarsal ulcers
When structural deformities like a dropped metatarsal head or thinning fat pad create excessive pressure on the ball of the foot, plantar ulcers often develop. These wounds are especially difficult to heal in diabetics with compromised blood flow and nerve damage.
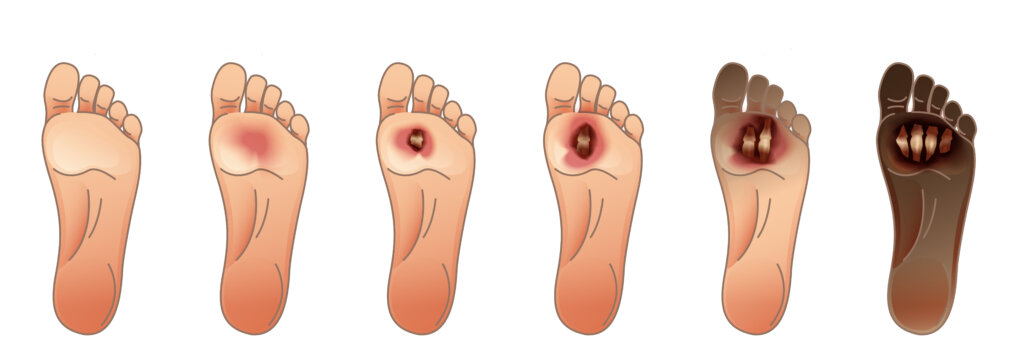
According to the Wagner-Meggitt Classification, these foot deformities are classified by these grades:
- Grade 0: The skin remains intact but some bony foot deformities result in the foot being considered at risk for developing an ulcer.
- Grade 1: A superficial ulcer develops.
- Grade 2: A deep full-thickness ulcer develops, extending beyond the dermis into subcutaneous tissue.
- Grade 3: A deep abscess forms, or osteomyelitis, which may also signal an infection.
- Grade 4: Partial gangrene of the foot occurs, localized in certain areas due to severe ischemia.
- Grade 5: The gangrene is extensive and involves the entire foot, which creates a high risk of systemic sepsis.
Minimally invasive osteotomies realign the metatarsal bones through small incisions, redistributing pressure and supporting ulcer healing. Two systematic reviews show that minimally invasive metatarsal osteotomies (MIMOs) are highly effective for healing plantar diabetic forefoot ulcers (PDFUs), with low recurrence rates and minimal postoperative complications.
Treating bunionettes
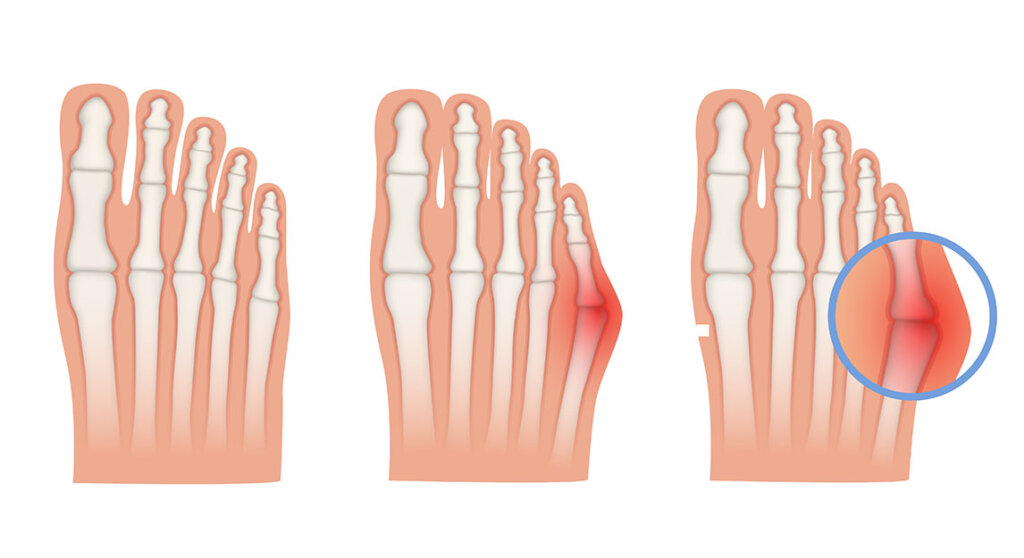
A Tailor’s bunion, or bunionette, is a bony bump on the outer edge of the fifth metatarsal. In people with diabetes, this deformity increases the risk of lateral forefoot ulcers due to constant pressure and friction.
Minimally invasive surgery can correct this by performing a distal or diaphyseal exostectomy, which reduces the bony prominence. This approach minimizes soft tissue trauma, allows early weight-bearing, and can be performed under local anesthesia, an effective option for high-risk patients.
Foot deformities: A small solution for a big bump
Exostosis refers to abnormal bony overgrowth, which can create pressure points that lead to ulcers, especially in weight-bearing areas. Diabetic patients are more susceptible due to poor circulation and neuropathy.
Minimally invasive exostectomy involves using a burr through tiny incisions to remove the bony growth with minimal tissue damage. This technique:
- Alleviates pressure
- Promotes healing
- Reduces recurrence
- Lowers infection risk
- Speeds up recovery
MIS addresses the structural cause of pressure injuries, making it a valuable tool in comprehensive diabetic foot care.
Charcot foot: Preserving structure
Charcot neuroarthropathy is a severe diabetic complication that causes foot deformities from joint dislocations and fractures, often leading to ulcers. Traditional open surgery is associated with higher complication rates.
MIS offers a safer alternative. In a case report, a patient with a plantar ulcer due to Charcot deformity underwent a minimally invasive exostectomy, which relieved pressure and led to rapid healing with fewer complications. This highlights the efficacy of minimally invasive exostectomy in patients with Charcot neuroarthropathy, demonstrating significant improvement in ulcer healing.
Minimally invasive techniques are reshaping diabetic foot care by providing safer, more targeted options for treating chronic wounds and structural deformities. From bunions and toe deformities to complex conditions like Charcot foot, MIS improves healing, reduces infection risk, and significantly lowers amputation rates.
Wound care certification empowers clinicians with specialized knowledge that helps identify, manage, and prevent complications associated with diabetic foot deformities. WCEI provides comprehensive education that helps clinicians develop a deeper understanding of wound pathology, while equipping them with evidence-based practices and confidence to deliver expert care.
This enhances their ability to integrate innovative interventions, such as MIS, that target the root structural causes of foot ulcers. MIS offers a forward-thinking, patient-centered solution in limb preservation, while also enhancing the overall quality of life for individuals with diabetes.
Elevate your expertise with education from WCEI!
Get StartedWhat do you think?